Preliminary Study to Develop the Korean Medical Pathologic Aging Scale and Korean Medical Pattern Identification for Dementia
Article information

Abstract
Objectives
To develop and investigate the reliability of the pathologic aging scale based on korean medical theory and korean medical pattern identification for dementia.
Methods
We searched the textbook of korean neurophychiatry and Donguibogam and selected items through professional consensus. We compared between dementia(n=40) and normal elderly(n=38) and tested the reliability of two scales.
Results
After professional consensus, we drafted the Korean Medical Pathologic Aging Scale(12 items, Likert 3 scale) and Korean Medical Pattern Identification for Dementia(4 patterns, 28 items, Likert 5 scale). On Korean Medical Pathologic Aging Scale, There is no significant difference between two groups. We had good internal consistency(Cronbach’s alpha = 0.6) and test-retest reliability(r=0.631) but low inter-rater reliability(r=0.430). On Korean Medical Pattern Identification for Dementia, dementia patients diagnosed with Qi deficiency are significantly more than those in normal group. We had fairly good internal consistency(Cronbach’s alpha = 0.574) and excellent test-retest(kappa= .800) and inter-rater reliability(kappa = .733).
Conclusions
Korean Medical Pattern Identification for Dementia is appropriate for diagnosing korean medical pattern. But Korean Medical Pathologic Aging Scale isn’t appropriate to discriminate dementia from normal elderly because of many subjective items. Therefore objective measurement of sensory dysfunction would be needed to measure pathologic aging based on korean medical theory.
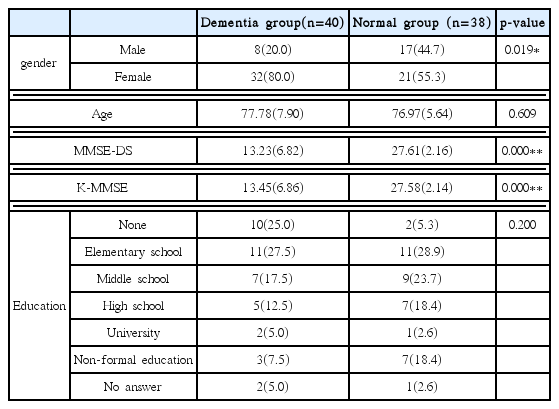
The Characteristics of Participants
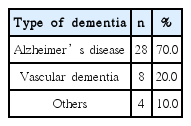
Type of dementia on Participants
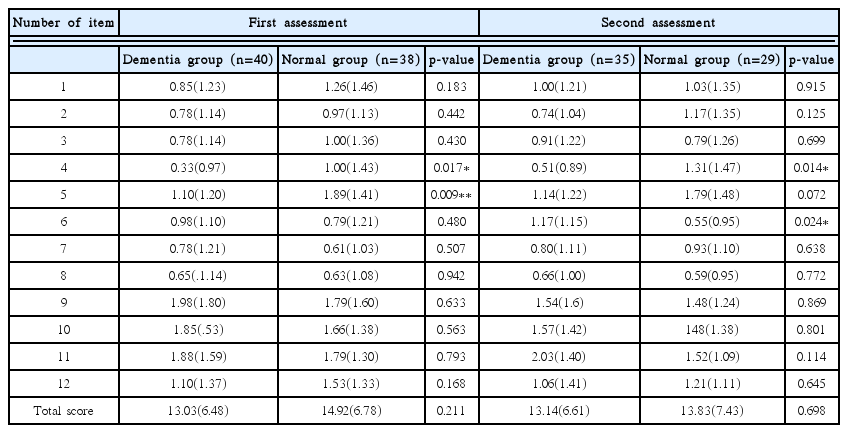
Comparison of Pathological Aging Scale Based on Korean Medicine between Dementia Group and Normal Group
Internal Consistency of Pathological Aging Scale Based on Korean Medicine.
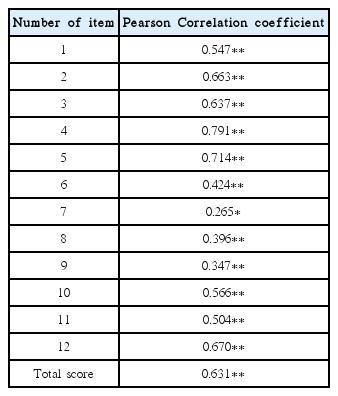
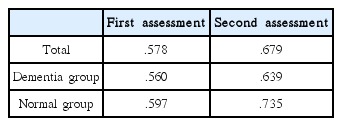
Test-Retest reliability of Pathological Aging Scale Based on Korean Medicine
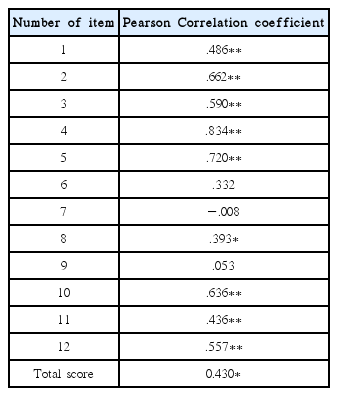
Inter rater reliability of Pathological Aging Scale Based on Korean Medicine
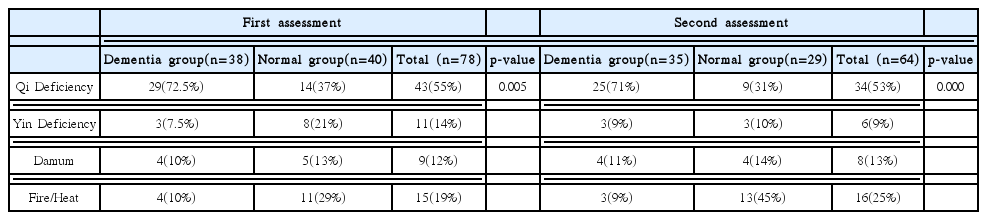
The Result of Pattern Identification Diagnosis of Dementia on Participants
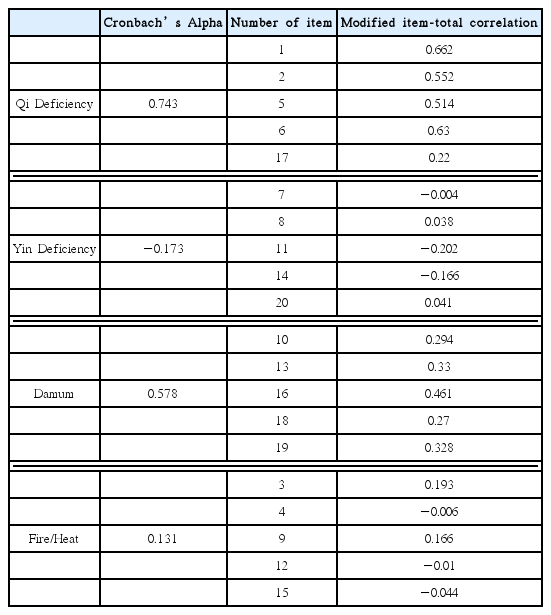
Internal Consistency of Pattern Identification Diagnosis of Dementia
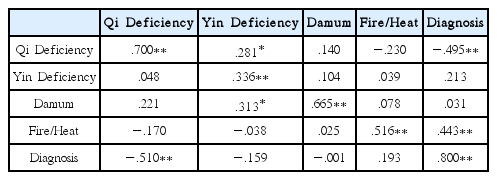
Test-Retest Reliability of Pattern Identification Diagnosis of Dementia
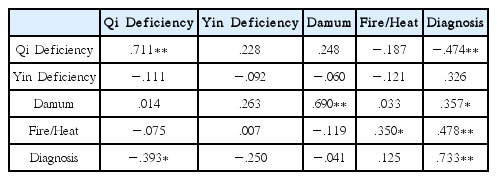
Inter-rater Reliability of Pattern Identification Diagnosis of Dementia
Acknowledgments
This study was supported by a grant of Ministry of Health & Welfare and the Traditional Korean Medicine R&D Project, Ministry of Health & Welfare, Republic of Korea. (HB16C0044)