Clinical study on recurrent Bell’s palsy: A retrospective observational study
Article information

Abstract
Objectives
This study is designed to statistically analyze characteristics, treatment effect and prognosis of patients who were treated for the recurrent Bell’s palsy
Methods
This study retrospectively analyzed the medical records and telephone questionnaire of 82 patients treated with the recurrent Bell’s palsy at the OO Korean Medicine hospital from August 01, 2018 to July 31, 2021.
Results
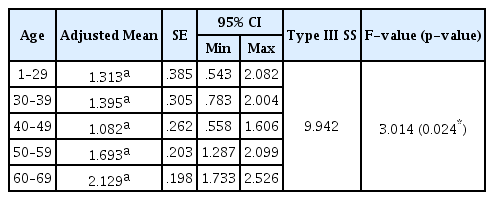
The lower the EQ-VAS® and HB scale before and after treatment, the higher the satisfaction with the treatment. The average of the number of days and duration of outpatient treatment for male was longer than that for female. The average number of days and duration of outpatient treatment in the group that received combined treatment was longer than that of patients who received Korean Medicine only. The higher the satisfaction of treatment, the higher the willingness to receive treatment in the event of recurrent facial palsy. HB scale after treatment was the lowest in their 40s, and the average value of HB scale after treatment tended to increase as age increased except for those in their 40s.
Conclusion
This study showed that the lower the HB scale after treatment, the lower the EQ-VAS®, the higher the treatment satisfaction, and the higher the probability receiving treatment if the facial paralysis recurs. Those in their 10s to 40s showed excellent results after treatment. Comparatively, those in their 50s and above showed a little effect after treatment. Gender, affected side, history of facial palsy, season of onset, age, hypertension and diabetes had no statistically significance with recurrent Bell’s palsy prognosis.
Study flow chart
HB scale before and after treatment
Adjusted HB scale after treatment

Frequency Analysis of Demographic Variables
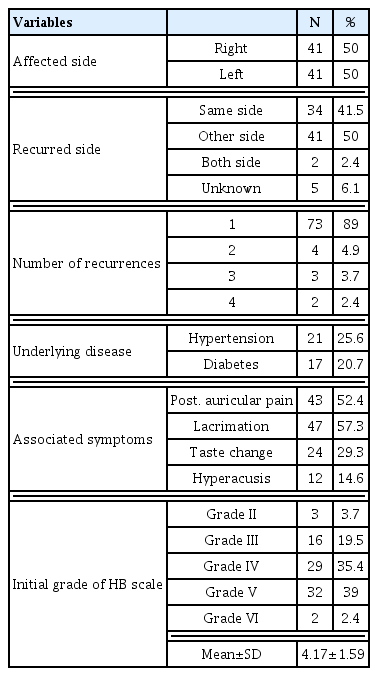
Frequency Analysis of Disease Variables

Frequency analysis of therapeutic variables
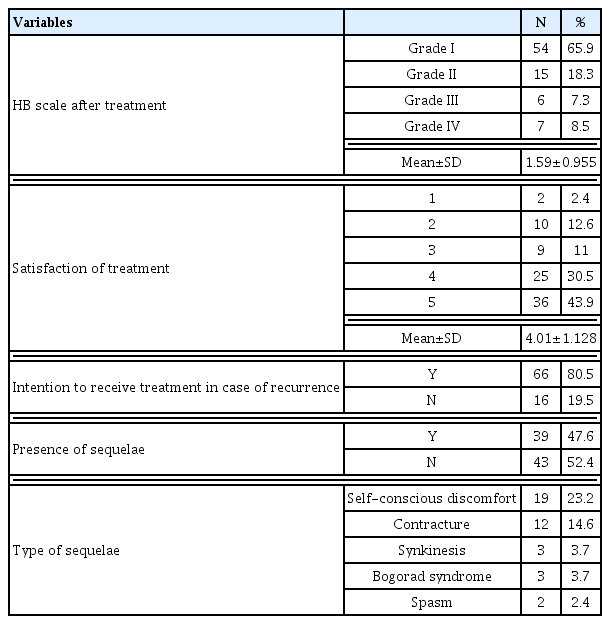
Frequency analysis and descriptive statistics of satisfaction characteristics
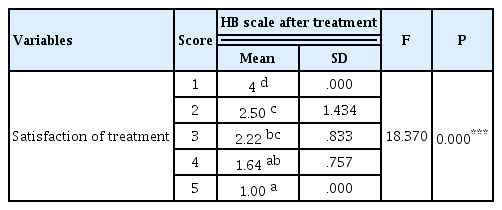
ANOVA of HB scale after treatment and satisfaction of treatment
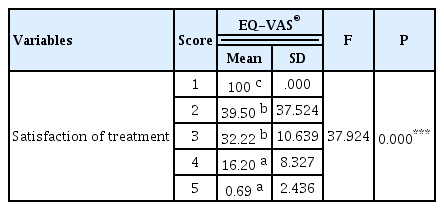
ANOVA of EQ-VAS® and satisfaction of treatment
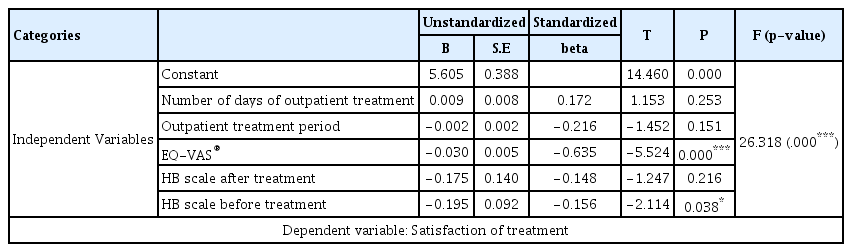
Multiple linear regression analysis of discharge satisfaction of treatment
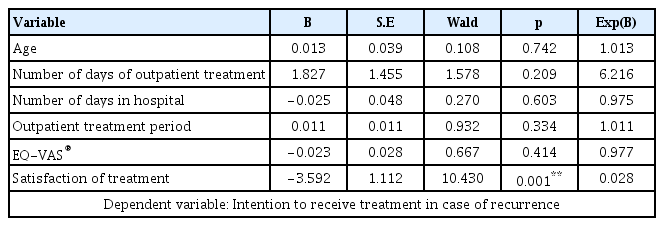
Logistics regression analysis of intention to receive treatment in case of recurrence
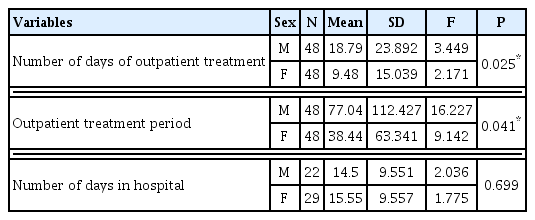
Independent T-test of difference between sex and number of days of outpatient treatment and outpatient treatment period
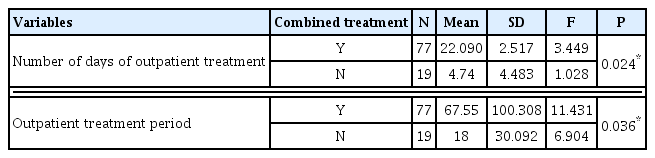
Independent T-test of difference between combined treatment and number of days of outpatient treatment and outpatient treatment period
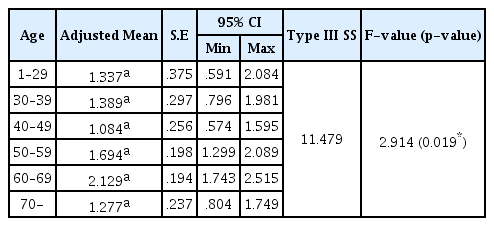
ANCOVA of HB scale after treatment and age
ANCOVA of HB scale after treatment and age 1 to 69